www.thetinman.org Copyright © All rights reserved.

Disclaimer: The material presented in this site is intended for public educational purposes only. The author is not offering medical or legal advice. Accuracy of information is attempted but not guaranteed. Before undertaking any diet, or health improvement program, you should consult your physician. The author is in no way liable or responsible for any bodily harm, physical, mental or emotional state of any patient reacting to any of the content on this site. Thetinman.org has not examined, reviewed or tested any product or service mentioned herein. We are not being paid to advertise or promote any product or service mentioned herein. The links are offered strictly as examples of resources available. The site assumes no responsibility or liability of any kind related to the content of external sites or the usage of any product or service referenced. Links to external sites were live at the time of creation of the link. Thetinman.org does not create content for or manage external sites. The information can be changed or removed by the external site’s administrators at any time and they are responsible for the veracity of their information. Links are provided to support our data and supply additional resources. Please report broken links to administrator@thetinman.org. Thetinman.org is not a charitable foundation. It neither accepts nor distributes donations or funds of any kind.

STIFF-BABY VARIANT
In childhood cases, it is important to rule out inherited hyperekplexia, sporadic and inherited dystonia, hereditary spastic paraplegia, and muscle rigidity in a newborn due to continuous peripheral nerve hyperactivity.
In multiple case reports, children exhibited rigidity of trunk and limb, hyperlordosis, startle reflex, and superimposed spasms. They showed continuous motor activity on EMG and responded to benzodiazepine treatment.
There have been onsets reported from ages six to sixteen. At the Mayo Clinic between 1984 and 2012, they identified eight patients with childhood onset ages one to fourteen. Five presented with classic SPS, two with stiff-limb, and one with PERM. Several were anti-GAD antibody negative. Intraoperative neuromuscular monitoring is recommended for children with stiff-baby variant.
STIFF-TRUNK VARIANT
Stiff-trunk syndrome is a rare occurrence associated with anti-GAD antibodies and evidence of other autoimmune disease. Stiffness and spasms are restricted to the trunk and spare the limbs. Rigidity of the trunk can become fixed over time making it difficult to bend or turn at the waist. It has a prolonged course but responds well to treatment with baclofen and benzodiazepines.
STIFF-LIMB VARIANT
A subgroup of patients present asymmetrically with stiffness and spasm primarily in one distal leg, which over time generalizes to both legs. A few cases involved the arms. Exaggerated curvature of the lumbar spine is absent. They may have abnormal fixed posturing of the hand or foot.
Patients generally present without the cortical or cognitive defects, seizures, and twitching jerks associated with other variants. The trunk is spared in the early stages. Most are anti-GAD antibody negative and do not exhibit other autoimmune dysfunction. Oligoclonal bands in the cerebrospinal fluid occur in a small percentage of those with the stiff-limb variant.
The stiff-limb variant presents with a distinct electrophysiologic picture. Electromyography shows continuous motor activity in the affected limb, but patients lack the symptoms, signs, and abnormalities attributed to the long tracts of the spinal cord. Cutaneomuscular reflexes are abnormal. As opposed to classical SPS, patients with stiff-limb syndrome exhibited exteroceptive reflexes and hypersynchronus segmented discharges during spasm.
Presentation of stiff-limb syndrome is more similar to patients with known focal pathology involving the grey matter of the spinal cord: intrinsic tumors, syringomyelia, vascular insufficiency, and paraneoplastic myelitis.
Up to fifty percent will develop sphincter involvement and thirty percent will develop brainstem involvement over several years. Brainstem symptoms include changes in breathing, difficulty swallowing food and water, problems with balance and movement, dizziness, and nausea.
Focal spinal lesions and infection are easily ruled out through imaging, microbiology, and serological studies.
Patient response to benzodiazepines and baclofen is mixed.
The stiff-limb variant runs a relapsing and remitting protracted course with sluggish progression over many years.
One out of four cases of stiff-limb syndrome develops into full stiff-person syndrome.
There is higher risk of becoming wheelchair or bedridden with this variant than with classical stiff-person syndrome.
There is some debate whether there are true variants or whether they are all different expressions of the same entity. However, there are patterns of presentation and progression that have earned their own titles.
JERKING-LIMB VARIANT
Jerking-limb syndrome presents in a tiny percentage of cases.
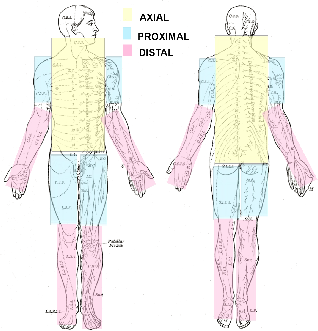
In addition to chronic muscle spasms, jerking-limb patients display rapid, violent, nocturnal or diurnal myoclonus (sudden, involuntary jerking of a muscle or group of muscles) lasting minutes to hours in the axial and proximal limb muscles. The jerks can be readily elicited by muscle stretch and touch to the perioral region. The spread of the twitching shows a rapid conduction upward through the brainstem and down the spinal cord. There are marked cranial nerve signs.
EEG-evoked responses precede the earliest response in sternocleidomastoids, are time-locked to jerks, and represent enlarged sensory evoked potentials.
The jerking muscles can appear many years into the course of illness and can involve all four limbs. In one case the stiffness and spasms preceded the jerks by nine years.
The symptoms respond well to diazepam.
Patients can present with stimulus-sensitive myoclonus even when the symptoms are otherwise well-controlled.
In a few cases it has progressed to seizures and lack of coordination.
Patients with the jerking-limb variant have survived more than ten years and have evidence of an autoimmune predisposition.
It has been suggested that jerking-limb is an early form of stiff-person syndrome with PERM. There is increasing evidence for a polioencephalomyelitis largely indistinguishable from that found in progressive encephalomyelitis with rigidity.
VARIANTS